
Understanding Parasympathetic Stress, aka the ‘Freeze’ Response, and Mobilization
What’s actually behind ‘paradoxical responses’ and ‘sensitivity to everything’, and why this is not a hopeless situation


The human nervous system has evolved over millennia to best support survival. It influences every function in the human body but its primary goal remains to manage energy resources to best support survival in the environment in which such evolution took place. While no-one disputes this summary, it is a symbolic of Western medicine paradigms that all treatments are provided without any consideration of the individual’s nervous system status and the impact this has on resource allocation; in other words, it gives no consideration to whether the person in question has a fair chance of responding to the intervention and instead follows centrally-issued guidelines on the ‘right’ drug to fix the diagnosis given. Equally, it is unfortunate that many alternative practitioners remain equally focused on external agents, albeit substituting pharmaceutical options for herbal choices.
It is therefore shocking-but-not-surprising that so many individuals spend years consulting with a long list of different practitioners and, while often accumulating a long list of labels and facing a growing inventory of contrived theories for their troubles, never have a single discussion as to the role their nervous system state may be having on progress (or lack thereof). It’s also why, when nervous system status is finally considered, one of the hardest things to comprehend is how the principles governing their trajectory are actually quite simple.
But, just because the principles are simple, this does not mean that the frontline steps required are easy. And the first step is to recognize how the nervous system is influencing our responses (and why, given the strained narratives that are spun to explain such reactions, we are prone to missing the big picture). To help with such orientation, let’s take a look at two journeys that serve us good examples of these scenarios, those of ‘Andrew’ and ‘Beth’.
Andrew’s Story
Andrew came to see me because, several months previous, he had come down with a viral infection; since this episode he had felt like ‘death warmed up’ and was so tired that he had been falling asleep at his desk if he didn’t drink coffee throughout the day. He had consulted his doctor, but was told that the tests showed he was ‘the picture of health’. He had tried anti-viral supplements but experienced no change. He found that a long run in the morning could make him feel ‘semi-human’, but that struggled to fit this into his day (he is an analyst for a trading firm and, when accounting for his commute, this required him to set his alarm for 5am). What’s more, he began to experience worsening back pain after each run; he’d seen a chiropractor several times but found that, while each adjustment provided relief at the time, any type of intense training would bring the pain back exactly as before. He came to me with the aim of ‘supporting his immune system so that he could finally clear the virus’.
After taking his case history, what stood out to me was the enormous stress that Andrew was under each day. Even when he wasn’t waking early to push himself on the treadmill, he was working long days in a highly demanding job in a stressful environment. In the past two decades, he had rarely slept more than 6 hours and said to me that any more than this was ‘too much sleep’; even when on holiday, he had avoided lie-ins because they made him feel so lousy. His Organic Acids Test revealed a range of areas across the board that needed support – specifically, energy metabolism, adrenaline output, inflammation and digestion – but it wasn’t the particular markers that caught my eye. It was the pattern of disinvestment that they painted (particularly the marker for malabsorption and the marker for downregulated thyroid activity at cell level), even more so in light of his Heart Rate Variability (HRV) readings (which he had been recording for some time using an Oura ring).
These readings, like every individual in a state of parasympathetic stress, were particularly high (apart from days in previous months when he did intense exercise, which would see it plunge into the 40s, it was consistently between 88-112; higher during the week, lower at weekends). This saw the over-simplified, non-contextualized daily readouts from his HRV app tell him that he was doing great generally but was more ‘stressed’ on Sundays (which was obviously a source of confusion). Combined with the fact that he didn’t feel stressed and the fact that he had lived a high-stress lifestyle for two decades without a problem, it was a challenge to explain that he was in a state of parasympathetic stress; in other words, that the stress his system was facing each day was so high that it was attempting to shut him down (ie. trying to ‘play dead’). The readings, the presence of the high adrenaline marker on the OAT and the fact he was (just about) able to function each day were all characteristic of a ‘functional freeze’ state. This is where key zones of the nervous system – specifically, the amygdala - is both mobilizing the sympathetic response in an attempt to meet demands, while other zones (brain stem) detect that the energy needs are too high relative to energy availability; as a result, it attempts a shutdown. These two competing actions result in this state.

Beth’s Story
Beth came to see me because she had seen a *whole host* of different specialists, both mainstream and alternative, over many years but without getting anywhere. She had a long list of symptoms, major brain fog, dizziness, bloating and difficulty digesting most foods and was ‘extremely sensitive’ to any supplements, which started to become an issue during a stressful period completing her degree at University but became her baseline immediately after completing her final exam, when she ‘crashed’. She had tried all manner of protocols, had seen thyroid specialists, gut specialists, heavy metal specialists, and the rest; almost all of them saw her experience worsening gut disturbances, inflammation, anxiety and sleep disturbances.
She was getting hopeless. Her many interactions with the mainstream system had simply resulted in prescriptions for antidepressants, which made her feel worse, and labels (‘functional neurological disorder’ and ‘dysautonomia’). Meanwhile, while she felt listened to by the array of alternative practitioners, none seemed able to handle the complexity of her issues or explain these ‘paradoxical’ reactions.
Beth’s Organic Acids test, as expected, showed the usual blend of challenges in energy metabolism, digestion (and, crucially, no marker for higher adrenaline production). It too showed low cellular activity of thyroid markers and markers for malabsorption. Her case history showed digestive issues from an early age and, most importantly of all, revealed that she was consuming far too little food, a total of only 1100kcals per day (which shocked her, as she was carrying some excess weight). One of the first things I asked Beth to do was to take her HRV measurements.
I did this more to quantify her current baseline and especially to provide clear evidence of what was happening. She explained that she was familiar with what it felt like to be stressed and anxious – as was the case for most of her teens – but that she had not felt this way for some time; this was now only something she felt after introducing supplements (particularly, those that supported energy production or that provided any calming effect).
However, I explained to Beth that there are two types of stress response, sympathetic and parasympathetic. The latter is rarely discussed, but a key characteristic is the way that individuals do not notice the fight-and-flight-type response. Other patterns that points to the parasympathetic stress include going through a team of specialists only to receive antidepressants and a diagnosis of ‘disorder/syndrome’ (check), encountered multiple theories that provided a one-stop solution for everything but never benefitted (check), early signs of autonomic nervous system disturbances, in this case digestion (check), major signs of reduced investment in digestive activity (check), getting fight-and-flight reactions whenever energy availability was increased or stress was reduced (check) and a tendency towards more pronounced reactions when correcting any nutrient shortage that had been shown on testing (check). Added to this, her HRV readings came in between 128-236 rMSSD, showing us that she was in ‘full’ state of parasympathetic dominance, aka ‘freeze’-type stress response.
Both Andrew and Beth’s stories have some substantial differences, there are certain things that bind them. They both had rational reason to think stress wasn’t a main contributor to their issues. They both had multiple responses that didn’t make sense. And they were both hearing about parasympathetic stress for the first time.
While my clientele clearly are not representative of the general population, around half the individuals I work with arrive in a state of parasympathetic stress. This type of stress response is clearly not uncommon, yet hardly discussed.
So what do we need to know about this? It helps to start by defining stress and how the human body handles this.
What is Stress?

We know that stress is bad for us. We often find ourselves in stressful situations. We understand that stress impacts on our sleep, digestion and mood. But what, exactly, is stress?
There are various ways we could define it. I choose this definition: stress is any circumstance where the resources we have are less than the resources we need.
The stress response is the physiological response that follows this, in order to bridge the gap in resources. The default response here is often dubbed the ‘fight-and-flight’ reaction, and sees our nervous system deploy a sympathetic stress response. The sympathetic nervous system is one of the two branches of our nervous system, and makes adaptive changes in our physiology to help balance this imbalance in resources. Its function can be distilled into three parts:
1. Reduced energy investment in non-emergency tasks (through withdrawal of vagal tone)
2. Increased mobilization of energy reserves from storage (through sympathetic nervous signals and the actions of adrenaline)
3. Increased opening of the gut lining to grab sugars and salts (through sympathetic nerve signals that activate transporter proteins within in the gut lining)
The combined effects of these steps are to moderately reduce energy demands while powerfully increasing energy availability to better meet the challenge. This is not bad, it is adaptive; however, such a response comes at a cost.
These costs can be divided into:
disinvestment in non-emergency processes – this includes digestion, detoxification, parts of the immune response and activity in key brain regions such as the prefrontal cortex (important for executive function, mood, memory and verbal fluency). This is mainly mediated by a withdrawal in vagal tone although, over the long term, our system may downregulate thyroid activity.
excessive alertness - something that may impact on mood, ability to socialise, find words and sleep. This is driven by both increases in adrenaline (which dials up activity in key brain zones that help with threat scanning) and withdrawal of vagal tone (which means less permission is given for activity in the zones used for social bonding and finding the right words)
inflammation and metabolic dysregulation – some inflammatory activity is instant, as the nervous system deliberately activates some immune populations (particularly the histamine-producing mast cells that protect the barriers of the body, pre-empting any flesh wounds). But more deep-rooted inflammation occurs over time due to the endotoxins that can now flood the bloodstream, driving up inflammation (especially nitric oxide) and downregulating hormone receptors (especially cortisol receptors). This reduced cortisol activity leaves us less able to control inflammation and regulate the stress response, while the nitric oxide competes with oxygen (limiting energy production). NOTE: nitric oxide is helpful when produced in the blood vessels, aka the endothelium (by endothelial nitric oxide synthase), but not when produced by the immune system (by inducible nitric oxide synthase).

What is Parasympathetic Stress?
As should be clear from the above, long-term stress can result in multiple costs that can drive a self-perpetuating cycle. The more inflammation and the less energy production, the more of an ‘energy gap’ (the difference between the resources we have and the resources we need). Accordingly, a bigger stress response is required to make ends meet. The more of a stress response, the more inflammation and the less energy production. Unless there is suitable intervention, the energy gap continues to grow and eventually cannot be bridged by the human stress response. At this point, our systems turn to its less preferred option; the parasympathetic stress response.
(Very important note: the above process describes how many individuals with chronic burdens reach a state of parasympathetic stress – ‘burnout’ over time. However, our systems may also be plunged through these stages directly into this state of physiological overwhelm in the case of acute trauma; there are some key nuances involved in supporting the nervous system and the exact neurobiology after such incidents, although the basic aims in providing support have little functional differences… nuances at the bottom of the article).
In any case, this deployment of parasympathetic stress is often described as a ‘crash’ and sees the individual in a state of shutdown that can be likened to hibernation. In this state, we feel foggy, tired, unmotivated and unable to switch on. Our heart rate drops, so too our temperature. We do not feel much emotion, just ‘bad’. Yet words to describe this are futile, just as they are to describe the fatigue. What is happening here is that areas of the brain stem, upon receiving sensory input that it interprets as an excessive challenge (one for which it can no longer sustain the fight required), it conducts a shutdown, using the parasympathetic nervous system to do so (for the precise neuroanatomy involved, see here; for a more functional discussion, see Steven Porges’ Polyvagal Theory).
The outcome is that the sympathetic response remains active but is over-ridden; arousal and defensive reflexes are inhibited, so too investment into all non-emergency activities. This has often been described as ‘playing dead’, and it becomes easier to see the evolutionary role of such a response when we realise that this comes with the release of endorphins to blunt both emotions and pain (which would be of great assistance in any overwhelming/threatening environment) and it will come as no surprise to those in a state of parasympathetic stress who can attest to feeling like ‘death warmed up’.
These neural mechanisms contribute to the other patterns and symptoms that we see in these scenarios. These involve a reduced motor control (one that often see the individual put through tests for Multiple Sclerosis), a flatness in emotional communication (mediated by lack of facial tone and reduced expression in the voice), difficulty in digesting foods (with bloating extremely common, with reduced release of intestinal secretions leaving individuals less able to break down food chemicals) and reduced detoxification. Although digestion is the most noticeable sign here, we see a maximal withdrawal of investment across the board (note: whereas fight-and-flight responses compromise investment in non-emergency tasks, freeze responses nearly entirely suspend it).
This is not a black-and-white scenario, as we will often see different levels of parasympathetic activity; sometimes a ‘full’ parasympathetic response (described as the ‘freeze’ response and one that features a full shutdown and comes with particularly high HRV readings, eg. 100-250 rMSSD) and sometimes a response where there is still competition between sympathetic and parasympathetic activity (dubbed ‘functional freeze’, where the individual in question can often maintain normal functions but feels a constant fatigue when doing so, and comes with HRV readings that are not as high, eg. 50-100 rMSSD).
But, regardless of the how strong the parasympathetic activity is, this naturally leads to an increasing range of symptoms, which naturally sees individuals keen to resolve them. Hence the pull towards SIBO treatment, anti-candida steps, heavy metal protocols and the rest. But, of course, none have a chance to work while the system is deliberately inhibiting investment in the zones necessary to respond.
How do we attend to Parasympathetic Stress?
There is only one avenue through which we can support someone in parasympathetic stress; through improving energy security, aka reducing stress (or, in more specific words, through reducing the gap between the resources we have and the resources we need).
This is not to say that there is a One Perfect Plan to deploy in these circumstances; in fact, the exact recommendations I provide can vary greatly. However, the principles never change and the main question I pose is always the same: what does this individual require to tend to their energy security?
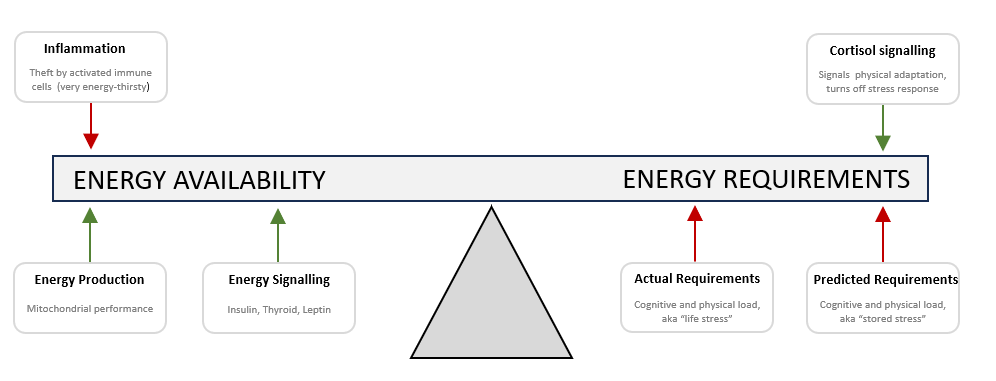
As readers may have picked up from my comments above, energy security can be viewed as an equation: how much energy resource we have, minus how much energy resources we need. If needs outweigh availability, our system mobilizes to bridge the gap; the problem is solved, albeit at an ongoing cost. If needs insurmountably outweigh availability, our system demobilizes (shuts down); the problem is not solved.
To keep things simple, energy availability is determined by three domains:
energy production (what is being produced in the mitochondria)
energy signalling (thyroid, insulin, leptin, etc)
energy theft (inflammation; activated immune cells are especially energy-thirsty)
Meanwhile, energy needs are determined by domains:
actual usage (work versus rest)
cortisol activity (which provides feedback to the control centres that ‘the body has adapted, you need not find more resources’, in doing so powerfully switching off the stress response)
predicted needs (where the ‘alarm centres’ of the brain, namely brain stem (ref) and amygdala (ref), continually predict a need for high readiness when no such need actually exists)
(NOTE: there are many ways that we could define stress and map out the drivers. It is not a case that this model is ‘right’ and others are ‘wrong’. But I find no other explanatory model that is both simple to grasp and applies to every single individual I’ve ever worked with).
So this is where a comprehensive case history and building a map of the day-to-day patterns can provide us with a clear idea of which of the six domains are playing a contributing role; the results of an Organic Acids Test can help us ‘work backwards’ to determine which step of which pathway is driving such issues.
Sounds simple, right? And, in principle, it is. But it is not necessarily easy, because of what happens when we do so.
Reduce the energy gap a little, so that it is no longer insurmountable, and the ‘emergency shutdown button’ is no longer pressed. We unfreeze. We are thrown back into the state of sympathetic stress, the one we experienced before the ‘crash’. This is a process known as mobilization and its rarely pretty.

Mobilization (and how it explains ‘paradoxical reactions’ and ‘extreme sensitivity’)
Mobilization lands us straight back in a state of fight-or-flight, and brings all the symptoms we would expect with it. As touched on earlier, this involves the liberation of energy reserves to flood the bloodstream (as well as grabbing them from the gut). It also comes with a spike in alertness. But it is also worth noting that, although any fight-and-flight reactions inevitably involve compromised investment across the body, this level of investment is far higher than is seen during the freeze-type responses. Why do I emphasize this small detail? Because any individual who mobilizes will see a sharp increase in activity in brain circuitry; this surge in neuronal activity can help with both the ability to think clearly but also with the transmission of sensory signals. The result? Your cortex becomes more active but, if there are any out-of-date rules held in the system – which is almost always the case - so too does your amygdala. People report feeling sharper, more alive and more resilient… but often more wired and agitated (especially ahead of bed, causing insomnia).
Not everyone notices anxiety. Some people will instead notice an increase in neuromuscular tension, aka ‘body armour’. I have discussed this pattern at length in a previous article (see “Pattern Four” in this piece), but is a form of reflexive bracing that result in blocking the transmission of sensory signals through the insula, the brain’s ‘relay station’ for passing emotional signals from the body to brain. What’s more, tension recruits a deep brain area known as the basal ganglia, which in turn deactivates the Default Mode Network (the network of our brain that scans for danger while we rest, activating the programmed emotional response when it receives any sensory pattern that has been associated with a need for readiness). This means that we feel no such rise in anxiety that is so characteristic of mobilization, but instead experience ‘unexplained’ symptoms. These vary based on where the tension occurs and can often appear as joint pain. However, we may see many other symptoms, depending on the location; if this tension manifests in the neck, expect headaches or tinnitus. If this is in the diaphragm, then expect a change in bloating (to a pattern that is now present upon waking, rather than one that builds after eating). Any tension that results in pressing on nerves can drive ‘unexplained’ tingling and irritation.
A spike in histamine is also common. The fight-and-flight response has evolved to help us not only engage in / escape from physical conflict, it also prepares us for the consequences; in particular, should the barrier of the skin be breached. This is where mast cells, the ‘first responder’ of the immune system, pump out histamine (to increase permeability of the local blood vessels, to allow for other components of the immune system to arrive and waste products to leave more feely). A further consequence is itching and increased sensitivity of nerve endings, which drives symptoms; the gut and bladder lining are rich in mast cells and , unsurprisingly, feature regularly in these patterns.
The takeaway? We add in an item that improves energy security and immediately notice unwanted symptoms. If applying the Western medicine paradigm – one that focuses on the treatment, rather than the individual’s physiology – then we will naturally conclude that “5-HTP ruined my sleep”, “Magnesium makes me inflamed”, or “B1 gives me headaches” , etc.
Dealing with Mobilization
Handling these issues comes down to three things:
introducing support at a slower rate
undertaking nervous system support
understanding what is happening
By nervous system support, I am referring to Breathwork, Somatic Experiencing, IFS/Internal Family Systems or similar. These approaches help to update any out-of-date rules held in the alarm centres of our system; this means that the sensory signals that have been unleashed during the mobilization process no longer need activate the amygdala and launch a fight-and-flight response. This means that we can now benefit from the increased neuronal activity, but without the stress response.
The pairing of a slower introduction of support with the nervous system work is key. This means that we are unleashing ‘bitesize’ waves of sensation, allowing our systems to remain within the window of tolerance; we no longer experience the ‘hijack’ of our system that would thrust our attention outwards instead of allowing us to remain introspective and, as a result, experience the sensations for what they are (which, after all, are just sensations). This process – experiencing sensations without anything bad happening - ‘proves’ to the alarm centres that no such fight-or-flight reaction is warranted. (NOTE: these alarm centres are fully capable of updating the rules they hold – this is neuroplasticity – but can only do so through experience rather than through cognitive reasoning).
It’s worth touching on the role of trauma here, especially given that this is a loaded word that may mean different things to different people. I feel trauma is best defined as ‘any experience that was a) overwhelming to the system and b) outside of our control’. This helps us to recognize three important things;
that there exists a spectrum of trauma, which has led to the increasingly popular concept of ‘little t’ trauma and ‘big T’ Trauma to delineate harsh-but-common life experiences (that leave their mark on almost all of us) versus more extreme events (be they accidents, assaults or bereavements)
that, as a result, residual overactivation of our alarm centres is almost universal (our questions are mainly guided towards assessing how this affects the system, rather than if it does)
that, although common, there does not need to be trauma in place for our alarm centres to hold some maladaptive/out-of-date reflexes
that a system with healthy energy resources and a functional stress response will often be able to maintain some degree of compensation for the high demands placed upon it; this is self-regulation. This may not create an ideal environment but it maintains stability. However, we cannot expect such energy resources or cortisol activity in any individual who has just started the mobilization process and, as a result, we cannot expect them to self-regulate
I’ve touched on the challenges that individuals with metabolic dysregulation face when trying to do the inner work in this article (which speaks of meditation, although the concepts apply to all inner work), but the takeaway message is that making using of external regulation is key. This means seeking support from a practitioner or in groups. The importance of this cannot be under-stated, as there is a huge difference in the outcomes we see when people connect with suitable support versus going it alone.
The third aspect to dealing with mobilization - recognizing what is happening here – is easily under-rated but has repeatedly proved vital in avoiding ‘secondary’ stress and anxiety; this refers to ‘the stress of being stressed’ and the ‘anxiety from being anxious’. This not only saves a lot of wasted energy and despair. It also allows us to remain in a more functional headspace when making choices on making our next steps (something that, if adrenaline output continues unabated, is easier said than done).

Andrew and Beth: Resolution
In Andrew’s case, a clear pattern emerged after we provided support. He felt better from digestive support (Digestive Enzymes), a mixed bag (better function but more backaches and insomnia) for energy support (which, was indicated on the Organic Acids Test, involved both Carnitine and B1) but experienced a ‘zombie-like’ state from anything that had a calming effect (most notably Licorice Root and Magnesium). This was consistent with his system dropping into a state of deeper parasympathetic stress (something borne out by the higher HRV readings).
I referred Andrew to a breathwork facilitator, with the aim of providing the Licorice in tactical/small doses ahead of a breathwork session. We first checked in on his response to the first session (which worked entirely on functional breathing patterns, which are often necessary in in order to benefit from the sessions that follow) and he then had his first ‘conscious connected’ breathwork. He reported a spectacular shift from this first experience; he felt a massive release of tension in the session and, while he felt generally unstable (with a lot of emotion bubbling up) in the aftermath, he also felt phases of ‘feeling alive’ in a way that he had not for a long time. He did experience some more incidences of poor sleep after providing further support but these were much less common and, when they did occur, much less pronounced. He was able to bring in the Licorice and Magnesium that previously saw him flatline and, after these were in place, he noted that he was now able to feel ‘fully awake’ in the day but not at the cost of sleep.
The biggest long-term win from the breathwork was that, by suspending his stress response during the sessions, he has a fair chance to observe (and feel) the effects that stress had on his system. As a result, he could now see what effects his daily schedule was having on his system. Although it took several months, he changed his job role, started to sleep for a lot longer each day and integrated some daily breathwork exercises into his routine. He noticed a lot of shifts in his system after this profound change in habits (including some major fluctuations in HRV readings which, as I explained, are entirely normal in these circumstances). This slower pace also meant that there was space to bring in items that may ‘take him down a notch’, and this is when I recommended Inositol. It is an item that is required in high amounts whenever the endoplasmic reticulum – the ‘protein factory’ of the cell – is put under stress (and it is placed under major stress during any viral infections, as viruses hijack this area to replicate themselves). It helps with neurotransmitter firing, immune function, insulin sensitivity and any process that involves protein synthesis (basically everything). When people bring this in after a phase where it had been low, they often feel a ‘smoothness’ that initially sees them quite sleepy. This is enhanced if there is any long-term sleep dept. It hit Andrew hard (in a good way) and he had a weekend where he did little but sleep, then slept 10+ hours for the week that followed.
However, he now felt increased baseline strength and then found that he had no further ‘unexplained’ reactions and, upon further retesting, the recommendations I gave him were integrated smoothly and his trajectory now unspectacular (in a good way).
Beth’s journey can best be described as a delicate dance, where we looked to exploit the options we had in order to generate a fair chance of responding to those that were to come (and to ultimately make a difference). We had a limited number of choices when it came to treatment, because of the issues with her digestion, appetite and reactions to so many foods. It is common for individuals with disturbed digestion to have a low appetite, something that becomes even more of an issue if their mobilization response involves a spike in histamine. Both applied to Beth.
She experienced hydrogen sulphide SIBO, which meant that higher-sulphur foods would reliably drive the formation of hydrogen sulphide (resulting both more bloating and brain fog). Therefore a full-spectrum digestive aid – ie. one that contained bile, a highly sulphurous substance – was unlikely to be a good fit. (It can also have implications on whether a ketogenic diet may be of assistance, as a high fat diet calls for increased release of bile). These reduced options are typical of the challenges faced by individuals who have been in ‘freeze’ for a long time; we needed her to eat more in order to provide more suitable signals to the nervous system (‘there is no longer a risk of starvation, you no longer need to hibernate’) but, while in this hibernation-type state, there was a pronounced lack of investment into the gut (which means chaotic environment and, normally, much less appetite). Using somatic approaches to break this cycle can often be a godsend, but tend to have limited effects while the individual is still subject to such low intake (it appears that evolution has determined that introspection is best avoided when we are in an overwhelming situation). Accordingly, although keen, Beth got little out of a breathwork session she attended.
Therefore, I suggested we focus on giving her the resources to successfully engage in these approaches. This started with a combination of Betaine HCL and an enzyme-only digestive aid. This helped; not quite enough but, alongside a low-ish FODMAP diet, allowed her to get near her closer to her caloric goals most days. But not all the way to these goals. I then recommended Cats Claw, an inhibitor of an inflammatory cytokine called TNF-a; aside from driving inflammatory symptoms, it also inhibits the neuropeptide orexin (which plays a crucial role in increasing appetite). If TNF-a is playing a role, we can expect this to make a different; if it is not, we cannot. However, after adding this, Beth was able to hit 1800kcals per day. She emailed me to say that she had finally noticed the responses I had told her to look out for… namely, the drop in HRV measurements and a return of insomnia (thankfully, by this point, we’d had enough discussions to know that this was a good sign).
Beth trialled a further breathwork session and, while she still did not feel that this had ‘moved the dial’, this was now doing something. She felt tension and pain in her abdomen. After a discussion of these patterns, what she felt about them and what felt confusing about them, I recommended that she connect with an IFS/Internal Family Systems practitioner. She found someone that she connected with immediately and she quickly began to look forward to these sessions, even though she would see unpredictable changes in the aftermath of each session.
Some of these changes were pleasant – eg. feeling genuine optimism for the future (for the first time she could remember) after one session, a huge growl and release in abdominal tension in another – but some were anything but. She had one particularly challenging phase where major histamine symptoms kicked in, alongside some terrible sleep (which, as anyone who has ever suffered with insomnia can tell you, makes any other challenges so much tougher than they already were). We took some measures to support sleep – Valerian Root, Lemon Balm and Lithium Orotate – as well as support for mast cells – extra Magnesium, use of Bicarbonate of Soda, Quercetin, breathing exercises to manage carbon dioxide levels (which she combined with an antihistamine). Their accumulative effect was not to entirely neutralize symptoms, but they did allow her to “just about stay sane” during the four weeks she needed them. Beth took heart from the fact that, even though her symptoms/sleep were by no means perfect in this time, she was actually getting improvements from a whole range of supplements (she was getting benefits, rather than ‘paradoxical reactions’).
This highly-activated pattern eventually ‘gave way’ and Beth then got some great sleep, with an occasional ‘aftershock’ that results in some bad night’s sleep. Her HRV readings were now very low (20-35 rMSSD), indicating a full transition into the sympathetic state. However, she now felt alive in the day time – no more brain fog or dizziness – and felt that she could now go about a ‘normal life’ (although was still liable to occasional bad night’s sleep and still had some bloating, albeit much less than before and could tolerate most foods now). She also found that she now got great responses when she trialled breathwork and she began to make use of this regularly. Most importantly, she no longer got ‘unexplained’ or ‘paradoxical’ reactions to supplements and was able to see gradual but reliable progress over the months that followed; though there were a number of ‘legacies’ to tend to first, we were eventually able to undertake the steps required to deal with lingering gut issues, especially bloating. HRV values slowly climbed, remaining entirely static after some changes and bouncing up in a pleasing way to others. The irony was not lost on Beth that the very steps she took in eradicating the SIBO/bloating issues were nearly identical to those that had failed so many times previously.
Takeaways
I hope the above makes clear several things about the parasympathetic stress response. Specifically, how common it is to see and how it explains many ‘unexplained’ issues but, most importantly, how recognizing what is happening here can allow us to provide suitable support and achieve predictable outcomes.
I also hope that this article makes clear that the principles involved in handling mobilization are always the same, but the steps required to do so will vary in different people (both in the metabolic support they need to come out of a ‘freeze’ state, and also in the processes called for to support their nervous system).
Most of all, I hope that the information above makes it clear that, while it is clearly normal to lose hope when we have tried so many things and seen such little benefit, these circumstances are far from hopeless.
Ps. Nuances
I have repeatedly spoken of the nervous system states as coming in three ‘flavours’; parasympathetic calm (‘rest-and-digest’), sympathetic stress (‘fight-and-flight’) and parasympathetic stress (‘freeze’). While it is indeed simpler to explain and simpler to grasp when nervous system states are divided up in this way, it is worth noting that there is a dynamic interplay between all three states, and that the mode of resource allocation that the nervous system deploys will always come down to the net sum of all three inputs. This most commonly affects the frontline responses in the case of ‘functional freeze’ (a scenario we encounter when there is both high
Many individuals will arrive in a state of ‘functional freeze’ for their first appointment and then quickly slip into a state of full ‘freeze’ when we provide effective support for their metabolism (especially in supplying support that helps regulate adrenaline production, such as Licorice Root and Magnesium). This can be thought of as a ‘failed freeze response’, where dysregulation of various neurotransmitters sees the sympathetic response (and subsequent adrenaline production) run amok in the midst of our systems trying to deploy a freeze response. Permitting healthier adrenaline regulation ends this ‘stand-off’ and allows the nervous system to enact the state it deems appropriate (which is always the preferred starting point for any successful journey)
the term 'freeze' is sometimes used in different contexts that relate to stressful and and threatening situations. Discussions on our reflexive responses to perceived threat often refer to the `4Fs': Fight, Flight, Fawn or Freeze. Such discussions can be very helpful to identify why we feel the way we feel during conflict (as well as teasing apart differences between instincts to throw down or run away), but the way these terms are used in this context relate more to innate threat-resolution strategy than autonomic nervous system state.
I have linked to a neurobiology paper above that describes how the brain stem is ultimately in charge of deploying the freeze response (specifically, the ventrolateral brain stem, which constantly receives information from across the brain but especially from the amygdala).traumatic episodes can thrust us into freeze via the brain stem-mediated mechanisms but also into a similar place via an alternative mechanism. In this whereby parts of the prefrontal cortex overly suppress the activation of the amgdala. This has been dubbed 'Freudian suppression'. It results in the same inhibited/numb state and the same high HRV readings. It also involves the same basic principles of a. providing more energy resources to allow for a bigger 'window of tolerance' and b. providing the nervous system support required. Individuals with this set-up may experience some differences in their journey, although the process (and the call to connect with a suitable practitioner) remains the same.
Thanks very much for sharing this, Marek. Very good information!